

Avalanche Response: Physiology, Rescue, and Resuscitation
THIS ARTICLE outlines the causes of morbidity and mortality in avalanche incidents, as well as prudent and practical rescue steps and medical treatments, based on the 2017 Wilderness Medical Society Practice Guidelines for Prevention and Management of Avalanche and Nonavalanche Snow Burial Accidents.
Avalanche risk can be mitigated by recognizing and avoiding dangerous condi- tions such as steep terrain (>30°), inclement weather, and an unstable snowpack. Formal avalanche education and mentored experience in avalanche terrain are the best ways to gain the required skills.
If caught in an avalanche, the top priorities should be getting off the slidingsnow surface and fighting to stay on top of the snow. If buried by an avalanche, one’s companions are the best hope for survival.
PATHOPHYSIOLOGY
The outcome of an avalanche burial is influenced by several factors, including thelength of time buried, whether the patient’s airway is open, if there is an air pocket, how deep they were buried, and if they were injured. The majority (75%) of avalanche fatalities occur due to asphyxia (lack of oxygen); a smaller percentage (25%) occur from traumatic injuries; and a very small number of victims succumb to hypothermia.
Asphyxia is caused by inhaled snow blocking the airway, the rebreathing of exhaled air, or an ice mask that forms over the airway after burial. Given that a lackof oxygen causes such a great number of fatalities, efficient extrication is key tothe patient’s survival. European research suggests that if the patient is extricated within 15 minutes, the chance of survival is greater than 90%. If the time of extrication extends to 30 minutes, the chance of survival plummets to 30%.
The specific injuries that account for the 25% of avalanche deaths from traumavary greatly. Most injuries are caused by collisions with trees or rocks or travel over cliffs. Asphyxiation is more likely to kill an avalanche victim before core temperature decreases enough to cause death from severe hypothermia. However, it is important to consider hypothermia due to its detrimental effect on other medical/traumatic conditions. Once the patient is extricated from the insulating snow, core tempera- ture can drop rapidly.
RESCUE
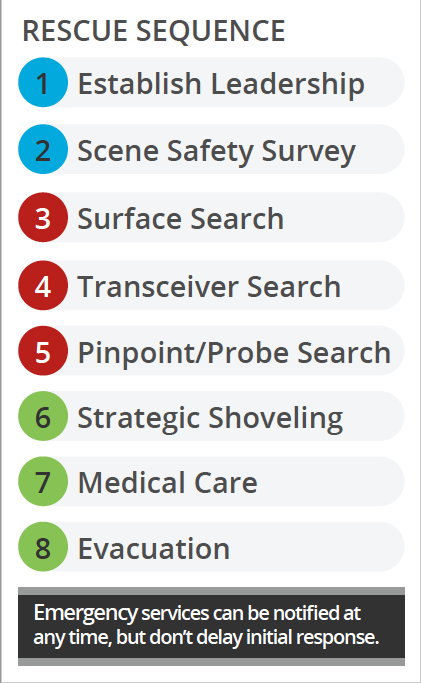
A systematic approach to avalanche rescue is of utmost importance. During an avalanche accident, rescuers should follow a rescue sequence, of which the key components are the establishment of leadership, a survey of the scene for risks to safety, a surface clue search, a transceiver search, a pinpoint (probe) search,strategic shoveling, medical care, patient evacuation, and the notification of emergency services. Depending on the number of available rescuers, individuals may be tasked with one or more elements of a rescue sequence.
RESUSCITATION AND FIELD TREATMENT
The International Commission for Alpine Rescue (ICAR) developed an avalanche victim resuscita- tion checklist aligned with the European Resuscitation Council (ERC) guidelines in 2010 and revised the original checklist in 2015. The ICAR checklist was developed to provide a methodical approach to medical treatment in an austere winter environment.
Survivability is influenced by a range of factors,including airway patency (airway open and free of snow or ice), burial duration, injury severity, core temperature, and the patient’s blood potassium level. Backcountry travelers with basic medical training should focus on basic life support (BLS).
It is important to note that no effective medical care can begin until the victim’s head and chest are fully exposed. Once extricated, all avalanche victims should be assessed for airway patency, effective breathing, and circulation.

If known, the burial time can help to dictate care decisions. The first step in medical care is to triage avalanche victims into two groups: those buried for less than 60 minutes and those buried for greater than 60 minutes. If resources are limited, care should be focused on those buried less than 60 minutes.
If vital signs (respirations and a palpable pulse) are present, basic first aid shouldbe administered as needed. This could include stopping any bleeding and splinting injuries. If vital signs are absent (no respirations and no pulse detected), rescuers should initiate cardiopulmonary resuscitation (CPR). For those buried more than60 minutes, the same steps should be taken. In addition, the first responder shouldnote if an ice mask was present in front of the victim’s face, suggesting an air pocket under the snow that allowed the patient to keep breathing for some time.
If basic life support (BLS) treatment does not result in the return of spontaneous circulation (return of a palpable pulse) after 30 minutes of resuscitation, further CPR is not necessary as the chance of survival is minimal. Responders also may take into account obvious lethal trauma.
The ICAR guidelines for advanced (ALS) treatment of avalanche patients are typi- cally reserved for trained providers with the necessary equipment. The checklist guides decision-making based on heart rhythm, core temperature, and potassium level. These steps are most appropriate in prehospital and hospital settings.
Dave Weber is a Denali mountaineering ranger and a flight paramedic for Intermountain Life Flight in Salt Lake City, Utah. Dr. Colin Grissom is a critical care physician for Intermountain Healthcare in Salt Lake City.

